The Risk Management Plan (RMP) documents the risk management system considered necessary to identify, characterise and minimise a medicinal product’s important risks.
The RMP should be updated throughout the life cycle of the product, for example;
if there is a change in the list of the safety concerns
when there is a significant change in the existing additional pharmacovigilance activities
if an emerging safety issue is confirmed.
The RMP should be assigned a new RMP version number and a date each time it is updated and submitted for assessment.
An updated RMP can be submitted as a standalone [currently C.I.11] variation, when necessary, but it is most often submitted as a consequence of or part of another variation.
The format and content of the RMP should follow the RMP template; Guidance on the format of the risk management plan (RMP) in the EU – in integrated format which consists of seven parts.
For a generic medicinal product, hybrid products and/or fixed combination products with no new active substance the safety concerns should be aligned to those of the originator product that are available;
either from the originator’s approved RMP
or from the list of safety concerns of the substance published on the CMDh website.
RMPs are approved per each medicinal product, not per MAH, therefore only one RMP should be submitted for an MRP or DCP with different MAHs. The RMP must remain identical in RMS/all CMS throughout the product life cycle.
The RMP should be provided in eCTD section 1.8.2. To facilitate the assessment a ‘tracked changes’ version of the RMP, in Microsoft word, should also be provided in the ‘working-documents’ folder outside eCTD.
The QPPV’s actual signature or the evidence that the RMP was reviewed and approved by the QPPV should be included in the finalised approved version of the document; for eCTD submissions this would be the RMP submitted with the last eCTD sequence of the procedure (usually the closing sequence).
Feel free to contact us here at ERA to assist you with all things regulatory in Ireland, UK and across the EU.
We take the pain out of regulatory so that you can take your medicine to the next level.
Written by
Fiona Downey
Fiona Downey 1
https://eureg.ie/wp-content/uploads/2014/08/pharma-vigilance.jpg262228ERAadministratorhttps://eureg.ie/wp-content/uploads/2023/10/European-Regulatory-Affairs-Logo.svgERAadministrator2024-07-19 09:53:292026-01-08 11:58:16Back to Basics – The Risk Management Plan (RMP)
In the EU, there are two different procedures available to apply for a marketing authorisation application (MAA) for the same medicinal product in more than one Member State at a time:
This Article focuses the Decentralised Procedure (DCP).
The DCP is only applicable if no marketing authorisation has previously existed in the EU/EEA, as per Directive 2004/27/EC andif an identical dossier is submitted simultaneously in all selected Member States.
To prepare for a DCP submission:
Establish a Reference Member State (RMS).
One Member State called the RMS will be selected by the Applicant to lead the assessment of the MAA.
To do this, complete a “Request for RMS in a Decentralised Procedure” Form and send it to your preferred RMS at least 2 months before the planned date of submission of the marketing authorisation application.
Only one RMS request can be submitted at a time. It is advisable to establish an RMS as soon as possible as DCP slots get booked up very quickly.
Prepare a dossier in accordance with the current legislation and EU guidelines.
Check that the requirements for submissions for new Marketing Authorisations are met for the various Member States to avoid validation comments (at Day -14) and also for any additional requirements to determine if any wet/original/notarised signatures are required
Ensure the correct fee amount has been paid.
Check the dossier for common validation issues raised by the RMS and the CMSs in DCP procedures to prevent them being requested during the validation of your application.
The applicant then simultaneously submits an identical dossier to the RMS and all CMS by the agreed submission date booked with RMS.
The application will be submitted via CESP portal, according to eCTD Guidelines, & then applicant will send any hard copies/original documents required by various Member States as per national requirements.
Assessment Reports (Day 70, D120, Day160, D210):
The RMS is responsible for preparing an Assessment Report (AR) which summarises the dossier presented by the applicant. The AR characterises and critically evaluates the medicinal product concerned with regard to its quality, safety and efficacy.
This AR will be made available to all Concerned Member States (CMS) together with SmPC, PL and labelling by the RMS and forms the basis for the evaluation by CMS.
In the case a Member State concerned by the procedure is unable to accept the AR or draft AR on the basis of a “potential serious risk to public health”, the application will be sent to the CHMP for arbitration.
End of Procedure can be in 90-210 days after validation phase is closed.
It is advisable to plan the national translations in time. It is critical that the translation service used is reliable and technically competent to translate medical text.
Seven calendar days after end of procedure the Applicant should send high quality national translationsof SmPC, PL and labelling and mock-ups to individual CMSs.
There is usually a 30-day National assessment before of the granting of the MA, however the timelines differ in each MS.
If consensus is not reached at the end of the procedure, a pre-arbitration (CMDH) and arbitration (CHMP) phase may take place.
https://eureg.ie/wp-content/uploads/2023/11/Legal-basis.jpg10002000ERAadministratorhttps://eureg.ie/wp-content/uploads/2023/10/European-Regulatory-Affairs-Logo.svgERAadministrator2024-06-17 17:33:012026-01-08 12:05:05Back to Basics – The Decentralised Procedure (DCP)
When an Applicant has a single marketing authorisation (MA) in one Member State and wishes to market the same medicinal product in other Member States in EU/EEA, a Mutual Recognition Procedure (MRP) can be used.
The Competent Authority where you hold the single MA acts as the Reference Member State (RMS) and the new Member States you chose are referred to as Concerned Member States (CMSs).
The RMS prepares the Assessment Report on the medicinal product and runs the procedure. The CMSs will raise questions during the procedure.
However, before you submit your MRP application, there are a number of things to consider;
You must ensure that the current dossier complies with the current legislation and EU guidelines. If your current dossier is not in line with the current legislation and EU guidelines it must be updated by variation prior to submitting the MRP application.
There must be no ongoing variations.
You must agree an appropriate time slot and request an updated Assessment Report (AR) from the RMS prior to submitting the application.
Each Member State will have a slightly different working procedure, but most require that discussions/requests start at least three months before your preferred starting time.
The RMS must allocate procedure number (e.g. IE/H/123/001/MR).
You must choose your CMSs carefully. Where applicable, review the approved legal supply status and local requirements (e.g. need for a local representative, local person for pharmacovigilance etc.) and reimbursement procedures etc. of each Member State.
If applicable compare the SmPCs of reference product across the interested territories, identify any differences paying particular attention to the indication(s) and posology.
The MRP follows by a 90-day period followed by a 30-day national phase.
To ensure that your MRP starts on time, it is advised to review the ‘additional data’ requirements of each Member State (e.g. do the cover letters, letter of authorisation need wet/original/notarised signatures etc?) and ensure the correct payment amount has been paid.
The CMSs can raise questions that relate to any aspect of the dossier from Module 1 to Module 5 such as issues with specifications, analytical validation, breakability data on scored tablets, process validation, biostudies including statistics applied to the studies, etc., all have to be addressed as “serious risk to public health”.
The CMSs are not allowed to ask for, and the Applicant is not allowed to supply, new data during an MRP.
Seven calendar days after close/end of procedure the Applicant should send high quality national translations of SmPC, PL and labelling and mock-ups to CMSs. It is critical that the translation service used is reliable and technically competent to translate medical text.
It is also important that the correct dialect or form of language is used. Due to this tight turnaround time, it is advised that discussions with your translator be performed in well in advance of the predicted Day 90.
The CMS should issue a marketing authorisation within 30 days after closure of the procedure, however in most cases depending on the Member State, this 30-day period is frequently missed.
Day Zero MRPs
A Zero Day MRP is an administrative RUP or MRP with a shortened timetable. A Day zero MRP is used in exceptional cases to mitigate shortages or issues with access to critical medicines in the new Member State.
In most cases the new CMS will not raise any quality or clinical question but will have specific criteria that need to be met prior to accepting a Day Zero MRP. The main prerequisite approval for a Day Zero MRP is that the medicinal product will be marketed in Member State as a result. Even though the procedure is administrative, the applicant should contact the RMS to agree on a submission date.
Countries like Iceland and Malta rely on such procedures due to the small size of the markets there.
Feel free to contact us here at ERA to assist you with all things regulatory in Ireland, UK and across the EU.
We take the pain out of regulatory so that you can take your medicine to the next level.
Written by
Fiona Downey
Fiona Downey 1
https://eureg.ie/wp-content/uploads/2019/07/Team-building.jpg360600ERAadministratorhttps://eureg.ie/wp-content/uploads/2023/10/European-Regulatory-Affairs-Logo.svgERAadministrator2024-05-31 11:45:532026-01-07 14:45:26Back to Basics – Mutual recognition procedure (MRP)
From the implementation of the Windsor Framework on 1 January 2025, the MHRA will regulate medicines across a UK-wide licensing regime.
Most new Marketing Authorisation Applications (MAAs) will be granted as PL licences covering the whole of the UK.
The MA number will have just a PL prefix (as it was before Brexit).
No action is necessary for this conversion for Marketing Authorisation Holders who only hold a PLGB licence for a particular product.
If a MAH currently holds both a PLNI and a PLGB for the same product and wishes to retain UK-wide authorisation, the PLNI will need to be cancelled in order for the existing PLGB to be converted to a PL.
Where an MAH only holds a PLNI and subsequently seeks authorisation for the whole of the UK, the PLNI will need to be cancelled prior to the granting of the PL.
MAHs involved in EU procedures, with NI included as a CMS, will need to notify the RMS to withdraw NI as a CMS from the procedure. This must occur before the cancellation of the PLNI and the granting of the new PL.
‘UK Only’ is required to be printed on the UK packaging from 01Jan2025, a sticker is allowed to be placed on packaging for a period of 6 months (until 30June2025) but this must be replaced with direct printing on the packaging after this.
And from 1 January 2025, the EU Falsified Medicines Directive (FMD) will no longer apply in Northern Ireland.
From 1 January features included for the purposes of compliance with EU FMD requirements may be removed or covered.
MHRA Overview:
Current position
From 1 January 2025
Action required from MAHs
New MAA for product in scope of the Centrally Authorised Procedure
GB: national applications, reliance/recognition applications,
PL
EC no longer able to authorise for NI.
For products entering the market from 1 January 2025, MAHs may apply for PL licences only. Must comply with labelling and packaging requirements.
New MAA for product in scope of the Centrally Authorised Procedure
NI: EC authorisation.
Supply of GB authorised products may be permitted through routes, e.g., NIMAR, Reg 174, Reg 167.
PL
EC no longer able to authorise for NI.
For products entering the market from 1 January 2025, MAHs may apply for PL licences only. Must comply with labelling and packaging requirements.
New MAA for Non-CAP product authorisations
UK-wide authorisation or option to apply for PLGB or PLNI
PL
Or
PLNI through the MRP/DCP
For products entering the market from 1 January 2025, MAHs may apply for PL licences or PLNI only if using the MRP/DCP. Must comply with labelling and packaging requirements.
Products with existing authorisations granted before 1 January 2025.
UK-wide licence
PL
Must comply with labelling and packaging requirements.
Products with existing authorisations granted before 1 January 2025.
Separate PLGB and PLNI for the same product.
Option A:
PL only
By 30 September 2024 the MAH should request that the MHRA cancel the PLNI, effective on 31 December 2024. PLGB licences will convert to PL by 1 January 2025.
Must comply with labelling and packaging requirements.
Products with existing authorisations granted before 1 January 2025.
Separate PLGB and PLNI for the same product.
Option B:
Retain NI only through the MRP/DCP.
No action required from MAH.
PLGB will be cancelled by the MHRA on 31 December 2024 as cannot hold a PL and PLNI simultaneously for the same product.
Must comply with labelling and packaging requirements.
Products with existing authorisations granted before 1 January 2025.
PLNI through the MRP/DCP, with no PLGB for the same product.
PLNI through the MRP/DCP only.
Where a MAH subsequently applies for a PL, the PLNI will need to be cancelled prior to the granting of the PL. The MAH should inform the RMS of its intention to withdraw NI as a CMS from the MRP/DCP.
Must comply with labelling and packaging requirements.
Products with existing authorisations granted before 1 January 2025.
PLGB only
PL only
No action required from MAH.
PLGBs will be converted to PL by 1 Jan 2025.
Must comply with labelling and packaging requirements.
CAP Bridging Mechanism
Permits supply of GB-licensed product in NI for up to 6 months if no equivalent available.
Not applicable as the MHRA will license novel/CAP medicines in NI through a UK-wide licensing route.
Not applicable.
Existing Stock in Existing Packaging on the market
Continues as currently.
Can continue to be supplied to patients until the product’s date of expiry in the territory for which the product was valid for supply prior to 1 Jan 2025.
Not applicable.
More on Windsor Framework in the weeks to come……
If you need any help to navigate this new min field of UK updates, don’t hesitate to contact us for support.
Written by
Emily Fletcher
Emily Fletcher 1
https://eureg.ie/wp-content/uploads/2024/02/Windsor-Framework-recd-13-02-24.jpg640960ERAadministratorhttps://eureg.ie/wp-content/uploads/2023/10/European-Regulatory-Affairs-Logo.svgERAadministrator2024-02-13 13:24:342024-02-13 13:25:45UK updates to your Medicine – Windsor Framework and Regulation (EU) 2023/1182
So, let’s start with the Legal Basis which forms the first step of your MA application (MAA for short). You need to know the legal basis before you can finish compiling your application.
The legal requirements and necessary procedures for submitting an initial application for an EU marketing authorisation (MAA) are set out in Directive 2001/83/EC, as amended, and in Regulation (EEC) No. 726/2004 (the latter for CP applications).
The legal requirements for a UK MAA are set out in the Human Medicines Regulations.
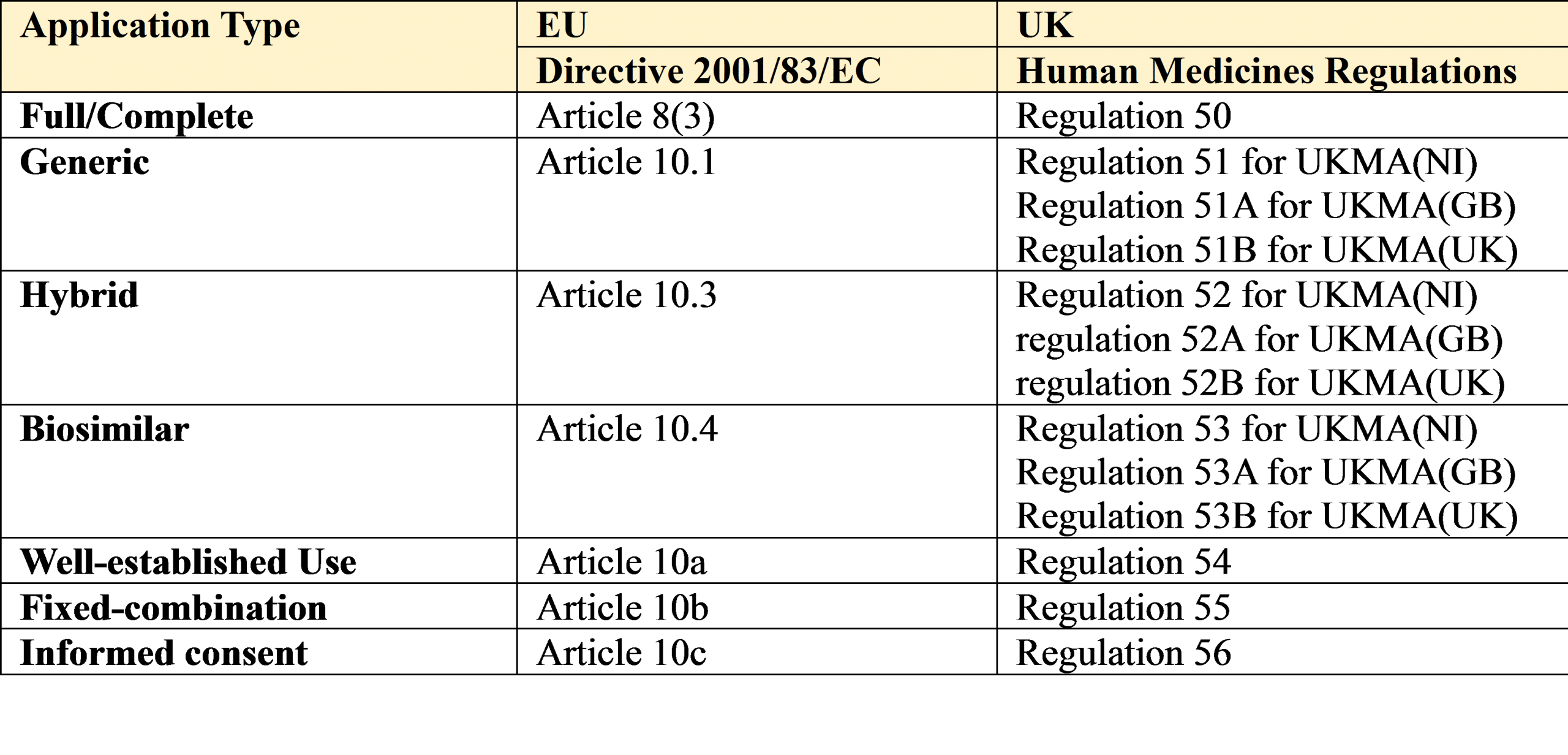
The relevant articles and regulations from this legislation are provided below followed by a brief description of each legal basis:
1. Full/Complete
An application for a marketing authorisation (MAA) must be accompanied by the particulars set out in Article 8(3) of Directive 2001/83/EC, as amended, and as well as all the usual documentation will also require the results of
• Physico-chemical, biological or microbiological tests,
• Pharmacological and toxicological tests,
• Full Clinical trials in human subjects
This Legal basis is most often used for brand new medicines (Drug Product) or active substances (Drug Substance) which have never been authorised in EU or UK before. It results in 10 years or 8+2+1 years of data exclusivity. No generic version can be marked until this exclusivity expires.
2. Generic
This is used when the medicinal product (Drug Product) for which an MA is sought is considered essentially similar to and interchangeable with a medicinal product that has already been authorised via Article 8(3) in the EU or UK.
Essentially similar means it has the same active substance, the same amount of active substance (strength), and the same pharmaceutical form.
In this case the Applicant cross refers to an already approved EU/UK reference medicinal product (RMP for short) to use its already approved data on the Pharmaco-toxicological and Clinical aspects of the application and so does not need to repeat these trials. Instead a bioequivalence study in human subjects is required. This data will show that the product is safe and works the same way inside the human body as the RMP does.
3. Hybrid
These are applications which rely on a mixture of data – i.e. a cross reference to the RMP for some aspects of the clinical and pre-clinical data requirement plus provision of additional data in support of any aspect of the proposed drug product which is different to the RMP (i.e. where it is not essentially similar).
This type of application is used when the proposed product has a different/new indication, different/new dosage form, different/new strength, etc. that is not currently approved for the RMP.
4. Biosimilar
These are generic products which are derived from a biological source rather than a chemically synthesised molecule.
It is often difficult to treat biosimilar generic products in the same way as we treat ‘regular’ generics as it is very tricky to prove essential similarity in the conventional ways – therefore provision of some preclinical and clinical data may be necessary to prove safety and efficacy of the biosimilar product.
The Guideline on similar biological medicinal products should be consulted when considering using a non-EEA authorised comparator (i.e. a non- EEA authorised version of the RMP) in the development of a biosimilar.
5. Well Established Use/Bibliographical
It is possible to replace results of pharmacological and toxicological tests or clinical trials with detailed references to published scientific literature if it can be shown that the drug has a ‘well established use’ with recognised efficacy and known safety.
The minimum criterion for using this legal basis of application is that the drug substance concerned has to have been marketed (i.e. in use) in the EU for at least 10 years. It is commonly used when no RMP exists to refer to or to perform a bioequivalence study against.
This type of application, although allowed for under the legislation, is not always accepted by member states (and they have been known to request clinical data, during assessment) but with the use of real-world data and evidence on the increase this type of application may become more common. Only Time will tell.
6. Fixed Combination
In the case of new drug products containing known active ingredients (drug substances), not before used in combination for therapeutic purposes, the results of pharmacological and toxicological tests as well as clinical trials in human subjects, relating to that combination, must be provided.
This legal basis covers entirely new products that are a mixture of two or more drug substances (sometimes called monocomponents), which have already been authorised and marketed in the EU in their own right. Because this is theoretically a full, stand-alone application (not unlike Article 8(3)), the product enjoys the full 10 or 8+2+1 years data of exclusivity.
Please note that the concept of the global marketing authorisation applies here so once a combination is approved any new application(s) for the ‘same’ product cannot be considered new combinations anymore and so an article 10b would not be acceptable in this situation.
7. Informed consent/Duplicate
The Marketing Authorisation Holder (MAH for short) of a complete/standalone dossier (i.e. the originator/innovator/RMP) can consent in writing to allow a new applicant/MAH to refer to the contents of their approved MA (on file with Competent Authority) for the purpose of obtaining a new MA.
The reference dossier must be a complete dossier (Article 8(3)) and consent must be obtained for all three modules containing the pharmaceutical (Module 3), preclinical (Module 4) and clinical data (Module 5).
The Applicant must choose the correct legal basis in advance of submission and selecting the wrong one will delay your application.
If you need any clarification or support contact us and we will gladly assist you.
If you are starting out in Regulatory Affairs and you now have a long list of questions after reading this article, we can help. We provide detailed training for all levels of Regulatory experience. You or your manager can contact us for details and our training menu.
Written by
Fiona Downey 1
https://eureg.ie/wp-content/uploads/2023/11/Legal-basis.jpg10002000ERAadministratorhttps://eureg.ie/wp-content/uploads/2023/10/European-Regulatory-Affairs-Logo.svgERAadministrator2023-11-23 20:50:292023-11-23 20:54:32Back to Basics – Regulatory 101 – Legal basis of your MA application in the EU and UK
The new veterinary regulation (NVR), Regulation 2019/6 applied to all EU Member States from 28 January 2022. The new legislation represents a significant change in how veterinary medicinal products are authorised, monitored and controlled in the EU.
The Regulation was developed in order to implement a fit-for-purpose veterinary legislation which would no longer be based on the equivalent human medicines authorisation system.
The new Regulation 2019/6 is broken down into the following chapters:
I. Subject matter, scope and definitions
II. Marketing authorisations
III. Procedures for marketing authorisations
IV. Post marketing authorisation measures
V. Homeopathic veterinary medicinal products
VI. Manufacturing, import and export
VII. Supply and use
VIII. Inspections and controls
IX. Restriction sand penalties
X. Regulatory network
XII. Common and procedural provisions
XII. Transitional and final provisions
Here is a summary of some of the noteworthy regulatory changes that have been introduced in chapters II, III & IV of the new veterinary regulation:
Chapter II – Marketing Authorisations:
An MA for a veterinary medicinal product shall be valid for an unlimited period of time. Hence, there is no longer a requirement for a renewal procedure or the sunset clause.
Chapter III – Procedures for marketing authorisations
Decentralised Procedure:
Scope and timelines remain unchanged
Responsibilities of RMS, CMS and applicant have changed at some steps of the procedure. For example,
– CMSs will also provide comments directly to the applicant at Day 100 and Day 145 instead of to the RMS only (therefore, comments are no longer anonymised).
– at Day 100-105 and Day 145-150, the applicant will now compile and circulate the LoQs.
– at Day 210, RMS will now be required to circulate a Final Assessment Report (FAR).
Scope remains the same. However, a minimum of six months is required between the decision granting the national MA and submission of an application for a MRP.
90 day procedure length remains unchanged but there are changes to some of the time-points in the procedure.
Responsibilities of RMS, CMS and applicant have changed at some steps of the procedure, similar to those outlined above for the DCP.
Centralised Procedure:
Scope of the mandatory use of the procedure has been widened. Refer to Article 42 (point no. 4) for details.
National Procedure:
No significant changes.
Subsequent Recognition Procedure (SRP):
Previously known as the “Repeat Use Procedure” is now officially recognised under Article 53 of the NVR.
Timelines and other requirements have been changed.
Due to the changes caused by the new regulation, CMDv have published updated guidance for DCP, MRP and SRP procedures:
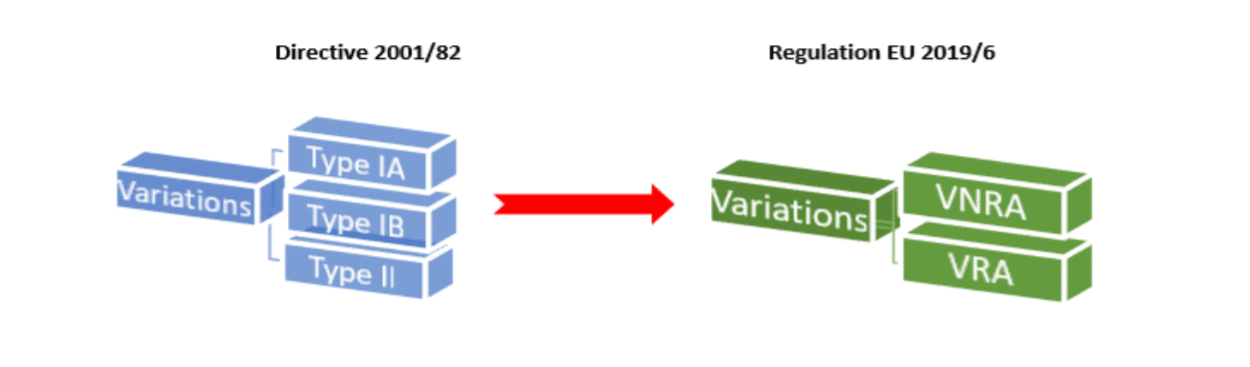
Chapter IV: Post marketing authorisation measures (Variations)
In terms of variations to marketing authorisations, one of the main changes arising from Regulation EU 2019/6 is that instead of the previous categories of Type IA, IB and II variations there will now only be two categories of variations:
Variations Not Requiring Assessment = VNRA
Variations Requiring Assessment = VRA
VNRAs consist of all the previous type IA and some Type IB variation categories.
VRAs will consist of most of the previous Type IB and all of the Type II variation categories.
Commission Regulation 1234/2008 will now no longer apply to veterinary medicinal products due to the introduction of new veterinary regulation (2019/6).
Variations Not Requiring Assessment (VNRA)
The Implementing Regulation (EU) 2021/17*, includes a list of all variations not requiring assessment along with any associated conditions and documentation requirements and is published in the EU Official Journal here.
The variations are classified as follows:
Administrative changes
Changes to the quality part of the dossier
Changes to the safety, efficacy and pharmacovigilance part of the dossier
Changes to the vaccine antigen master file (VAMF) part of the dossier
VNRAs will be processed as follows:
The MAH will:
– Record the change in the Product Union Database (UPD) within 30 days of implementation including required documents (no application form is necessary).
– Documents submitted directly to UPD. No CESP submission. Documents include those listed in the Implementing Act as well as SPC, package leaflet, labels.
The relevant CA/RMS will
– Approve/reject the variation
– Inform MAH & CMS by recording decision in database and by e-mail
The format and categorisation is similar to the previous regulation which applied (Commission Regulation 1234/2008 ), however there are many differences.
The variations are divided into chapters as follows:
E. Administrative changes
F. Quality changes
G. Safety, Efficacy and Pharmacovigilance changes
H. VAMF or, PTMF changes
I. Changes of active substance(s), strength, pharmaceutical form, route of administration or food producing target species
Z-categories have also been included to address unlisted variations and VNRA, if requirements laid down in the Implementing Regulation are not met.
The timetable for VRAs is also outlined in the new guidance as follows:
a standard timetable, denoted by ‘S’ which will be 60 days
a reduced timetable, denoted by ‘R’ which will be 30 days
an extended timetable, denoted by ‘E’ which will be 90 days
For details on how to submit a VRA, CMDv have written a Best Practice Guide for Variations Requiring Assessment (EMA/CMDv/144277/2021). It has been prepared in order to facilitate the processing of VRAs for MRP/DCP products. The same general principles will apply to purely nationally authorised products.
Recommendation for the classification of variations not already listed
A procedure for requesting a recommendation for the classification of variations not already listed in either the above-mentioned Implementing Regulation or the EMA/CMDv Guidance on variations requiring assessment has also been established. This is similar to the previous CMDv recommendations for classification of unforeseen variations, according to Article 5 of Regulation 1234/2008.
Grouping and worksharing procedures do not apply to VNRA, they only apply to VRA.
As a consequence, no VNRAs can be included in a grouping or worksharing even if they are consequential or related to the VRAs included in the grouping or worksharing procedure.
However, the introduction section of CMDv Best Practice Guide for Variations Requiring Assessment (which also covers grouping), outlines the different approaches to follow when there is a need to co-ordinate changes that are related or consequential but are classified as VNRA and VRA.
The worksharing procedure is outlined in Article 65 of the NVR and it will be compulsory to follow this procedure, when the same change is being applied in different member states. Information related to worksharing is also mentioned in the CMDv BPG for Variations Requiring Assessment. However a specific guide on worksharing has also been written by CMDv: Best Practice Guide for Worksharing (EMA/CMDv/204024/2021).
Union Product Database
Due to the new regulation, the EMA has introduced new IT systems. The main one will be theUnion Product Database (UPD).
It will contain information for all authorised veterinary medicines in the EU (including all nationally authorised products). For MAHs, it will provide self-service access for specific regulatory activities, including the management of variationsthat do not require assessment.
For more information on implementation, training, registration and access of the UPD, refer to the following link here on the EMA website.
The UPD will be linked to the other 3 other databases in the future. These databases are at different stages of development and introduction:
Union Pharmacovigilance Database
On 28 January 2022, the Union Pharmacovigilance Database (EVV) was successfully released. User guidance and the release notes are available here.
Manufacturing and Wholesale Distribution Database
The Manufacturers and Wholesale Distributors database (MWD) was released on 28 January 2022. The system is an enhanced and upgraded version of EudraGMDP, the EU database of manufacturing authorisations and certificates of good manufacturing practice, with changes affecting both the veterinary and the human domains. The MWD Project Group has also adopted requirements for aligning the GDP module with the change made to the system so far. Changes to the module will be delivered in a subsequent release scheduled for Q1 2022. In addition, enhanced search facilities on the GMP module will be delivered in the same release.
Database for the Collection of Data on Sales and Use of Antimicrobials in Animals.
IT development on the Collection of Antimicrobials Sales and Use Data (ASU) project started in January 2022. Information on the progress of this project will be published on the EMA website as this project develops.
Q&A on transitional arrangements
CMDv has prepared a Q&A document in order to assist both MAHs and NCAs in the management of the transition between the requirements of Directive 2001/82/EC and Regulation (EU) 2019/6. This Q&A document will be regularly updated and can be found under the following link.
This document includes an Annex which outlines how individual Member States will handle renewals of marketing authorisations after 28 January 2022.
Should you need any support with Veterinary Procedures feel free to contact us & the Ivowen team will be here to help.
Written by Claire Brown
https://eureg.ie/wp-content/uploads/2022/04/Vet-article-feature-image-05-04-22.jpg6221106ERAadministratorhttps://eureg.ie/wp-content/uploads/2023/10/European-Regulatory-Affairs-Logo.svgERAadministrator2022-04-05 12:52:052023-11-06 11:18:32The new veterinary regulation (Regulation 2019/6) and its implications on regulatory submissions for veterinary medicinal products
There are now several routes to obtain a marketing authorisation in the United Kingdom (UK), Great Britain (England, Scotland and Wales) or Northern Ireland. The options available will be determined by the intended market and the type of application. In this article we will discuss the purely National procedure.
To help you to decide what type of license you will require, here is a brief explanation of the new types of MA you can obtain:
MA prefix for UK
Possible MA types
Territory
Leg & Guidance
PL
UK wide
Authorised for use in United Kingdom (Great Britain & Northern Ireland)
EU & MHRA rules apply
PLGB
GB
Authorised for use in Great Britain only (England, Scotland and Wales only)
MHRA rules apply
PLNI
NI
Authorised for use in Northern Ireland only
EU rules apply
One option you can pursue is the National procedure (a 150-day procedure) to obtain a marketing authorisation (MA) in the UK, Great Britain or/in Northern Ireland. The MHRA has introduced this accelerated procedure aimed at expediting the availability of medicines for patients in the UK and proposes to reach its opinion on marketing authorisation applications (MAAs) within 150 days of filing an application (excluding the time taken to provide further information or data required).
The accelerated assessment is available for all high-quality new MAAs for both new, and existing active substances, as well as orphan designations. Interested applicants should contact the MHRA in advance of submitting the application.
For medicines containing new active substances or biosimilar products, the MHRA encourages applicants to provide a summary of the dossier to share their intentions and to verify the new active substance status.
The pre-submission meeting offers the opportunity to discuss the arrangements for the UK Compliance Check (CC) on Paediatric Investigation Plans (PIPs). Additionally, it also offers the opportunity to enhance joint discussion with National Institute for Health and Care Excellence (NICE) Health Technology Assessment (HTA) evaluation process.
The MHRA will operate a ‘fixed submission date’ system to facilitate consultation with the Commission on Human Medicines (CHM) and will publish a set of dates to facilitate planning the submissions to coordinate with appropriate meeting dates of CHM. The submission slots will be linked to the dates of CHM meetings.
The assessment timetable will begin after the validation of the application. The assessment process will run in two phases totalling 150 days like so:
Phase I: completed 80 days after the clock starts. Issues that arose or requiring clarification from the initial assessment will be raised with the applicant and should be addressed within the clock off period of 60 days.
Phase II: commence on receipt of the applicant’s responses. The MHRA will provide a decision on the acceptability of the product by day 150.
If the MHRA refuses to grant the MA-based on advice from CHM, there is an opportunity for the applicant to request a review of the decision.
The conclusion of the assessment will lead to the publication of a UK Public Assessment Report for the product.
Here are some useful links to obtain further information:
If you need any clarification or support to help you to navigate the new post Brexit procedures, please contact us and Ivowen will gladly assist you in a timely manner.
https://eureg.ie/wp-content/uploads/2019/01/Brexit2.jpg413640ivowenadminhttps://eureg.ie/wp-content/uploads/2023/10/European-Regulatory-Affairs-Logo.svgivowenadmin2021-04-21 13:25:462023-11-06 11:15:36New UK National Procedure – Expedited 150 day procedure
The UK has left the EU and the transition period after Brexit comes to an end this year.
The MHRA have issued new guidance for industry and organisations effective from 01st January 2021. From this date the MHRA will be the UK’s standalone medicines and medical devices regulator.
Areas covered in the new guidance include:
Clinical Trials
From 1 January 2021, for registering clinical trials, existing and established international registers will still be used, such as ISRCTN registry (UK), or ClinicalTrials.gov (USA), to ensure the public is aware of your trial. For trials involving both UK and EU sites a record in the EU Clinical Trials Register will exist (other than adult Phase 1 studies). In the UK, any favourable opinion given by a research ethics committee is subject to the condition that the clinical trial is registered on a publicly accessible database. The time frame for publishing the summary of results is within 6 months of the end of trial for paediatric clinical trials or within one year of the end of trial for non-paediatric clinical trials. You do not need to submit this clinical trial summary report to the MHRA as well; however, you must send a short confirmatory email to CT.Submission@mhra.gov.uk once the result-related information has been uploaded to the public register and provide a link.
Pharmacovigilance
Guidance on qualified person responsible for pharmacovigilance (QPPV) including pharmacovigilance system master files (PSMF) from 1 January 2021
From 1 January 2021, the following legal obligations will apply to holders of UK marketing authorisations (MA). These include those that cover the whole of the UK, or are specific to Northern Ireland or to Great Britain (England, Wales and Scotland):
To operate a pharmacovigilance system for UK authorised products.
To have an appropriately qualified person responsible for pharmacovigilance (QPPV) that resides and operates in the EU or the UK and is responsible for the establishment and maintenance of the pharmacovigilance system for UK authorised products.
To maintain and make available upon request a pharmacovigilance system master file (PSMF) that describes the pharmacovigilance system for UK authorised products. The PSMF must be accessible electronically or physically from the UK at the same site at which reports of suspected adverse reaction may be accessed.
Statutory guidance concerning the QPPV for UK authorised products is described in the Good Pharmacovigilance Practices (GVP) Module I. This guidance will be supplemented by the ‘Exceptions and modifications to the EU guidance on good pharmacovigilance practices that apply to UK marketing authorisation holders’, which will be published in due course.
New guidelines have been outlined for Marketing Authorisations, to include Conditional MAs, registering new packaging information, guidance on the handling of applications for Centrally Authorised Products (CAPs), Article 29 applications, converting parallel distribution notices to UK parallel import licences, handling of ASMFs and CoS from January 2021, reference medicinal products, converting CAPs to UK MAs, guidance on licencing biosimilars, bioequivalence/therapeutic equivalence studies and renewing marketing authorisations.
New Submission Registrations
For planned applications for submission to the UK (for example, a Marketing Authorisation for the UK market), you will need to submit the information through the MHRA national portals.
All current Eudravigilance Gateway users who wish to gain access to the new MHRA Gateway will need to first gain access to MHRA Submissions. The steps for gaining MHRA Gateway access are contained within MHRA Submissions. MHRA Submissions will not be used to send or receive ICSRs.
If you need any clarification or support to help you to navigate the end of transition period please contact us and Ivowen will gladly assist you in a timely manner.
Written by Mary Canning
https://eureg.ie/wp-content/uploads/2020/07/Brexit-clock-image-22-07-20.jpg422750ERAadministratorhttps://eureg.ie/wp-content/uploads/2023/10/European-Regulatory-Affairs-Logo.svgERAadministrator2020-11-06 12:15:002023-11-06 11:15:33BREXIT – MHRA post-transition period information
Did you know, that pharmaceutical companies can consult the European Medicines Agency (EMA) to determine whether a medicine they are developing is considered an advanced therapy medicinal product (ATMP)?
In doing so, they are allowed to receive confirmation that a medicine, which is based on genes, cells or tissues, meets the scientific criteria for defining an ATMP. The criteria for ATMPs are set out in Article 17 of Regulation (EC) No 1394/2007.
In order to submit an application for ATMP classification, applicants have to complete a:
pre-submission request form
ATMP-classification request form and briefing information
and return both forms to the EMA.
Applies to your company? Ivowen are here to assist you.
For more information on Ivowen’s services and how we can help you, contact us.
Firstly, in this very unusual time for us all I want to let you know that our dedicated team are all healthy, safe and working from home, business as usual, to ensure that we continue to provide you with the high quality and efficient service you have come to expect from Ivowen.
Have you ever wished you could get the opinion of an Assessor before you go to the National Competent Authorities with your queries?
Well, I am delighted to introduce you to to our newest team member Claire Brown.
Claire has come directly to Ivowen from the Health Products Regulatory Authority (HPRA) and brings with her a wealth of experience as a pharmaceutical assessor of human medicinal products. Claire has been part of the team here in Ivowen since 2019 and has more than 12 years experience working in the HPRA. She started there as a Scientific Officer working mostly on veterinary medicinal products and was promoted to Pharmaceutical Assessor after 3 years.
Claire completed her undergraduate work in Chemistry and her postgraduate work in Neuropharmacology and Industrial Pharmaceutical Science.
Claire adds her extensive experience to our knowledgeable team so that we can enhance the services we provide to you and continue to give you an ‘Assessor’s eye’ opinion on your applications before you submit them.
I invite you to visit our updated Meet the Team page to see all the talented people who enable us to guide you through all aspects of regulatory strategy, dossier preparation, MA submissions through to national phase, post-approval variations, product development, quality overviews, medical devices and much much more.
If you could use some assistance to navigate the complex world of regulatory, please feel free to contact us for further information.
Written by Alice D’Alton.
https://eureg.ie/wp-content/uploads/2014/09/pharmacovigilance2.jpg3471080ERAadministratorhttps://eureg.ie/wp-content/uploads/2023/10/European-Regulatory-Affairs-Logo.svgERAadministrator2020-03-31 19:02:032023-11-06 11:08:10How to get an Assessor’s opinion before you contact the Competent Authorities